A 40 yo lady arrives in ED by ambulance with neck and spinal immobilization because she fell down a staircare.
The patient’s vital signs are within normal physiological parameters, she is alert, no deficit, remembers all, denies head contusion and neck pain. She complains for a sharp shoulder pain (NRS 10/10), it seems broken.
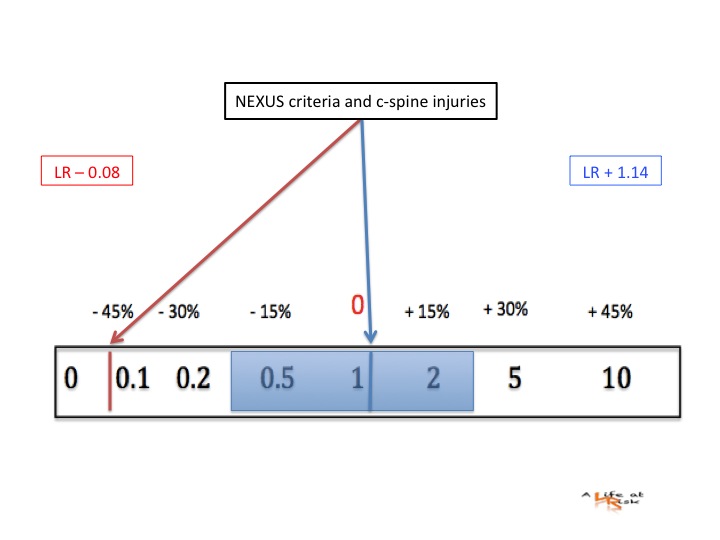
If I perform the Nexus C-Spine criteria X Ray is indicated: a distracting injury mandates cervical spine imaging.
How much the presence of distracting injury reduces my sensibility in rule out cervical spine (c-spine) injury?
Conclusion
Once upon a time nearly all patients who presented in ED with blunt trauma received a cervical spine X-Ray. The clinicians feared to undiagnosed a cervical fracture, with catastrophic consequences for the patients and than for the same doctor, so there were a large number of unnecessary films. The Nexus five criteria simplified our work: it’s easy and speedy and especially is high sensitive to rule out a cervical spine injury. The presence of a distracting injury has a negligible impact.
Is it time to define the Nexus four criteria?
Bibliography
MK Rose
Clinical clearance of the cervical spine in patients with distracting injuries: it is time to dispel the myth.
J Trauma 2012 vol 73 n 2 pag 498-502.
A Kostantininidis
The presence of a nonthoracic distracting injuries does not affect the initial clinical examination of the cervical spine in evaluable blunt trauma patients: a prospective observational study.
J Trauma Sept 2011 vol 71 n 3.
Paucis Verbis: distracting injuries in c-spine injuries from Academic Life In Emergency Medicine Sept 2011.