A 53 year old man is involved in a motor vehicle crash. He refers a moderate thorax and abdominal pain. No head injury, the helmet is not broken, the patient remembers the accident. Systolic blood pression is 120/80 mmHg, respiratory rate is 24, saturation is 100%, he has abrasions over the torso and right thorax and flank, no wounds. The eFAST shows a normal pleural sliding, and no signs of intraperitoneal blood.
The institutional blunt trauma protocol requires an arterial blood gas (ABG) and serum lactate (SL), than is obtained a CT of the chest abdomen and pelvis.
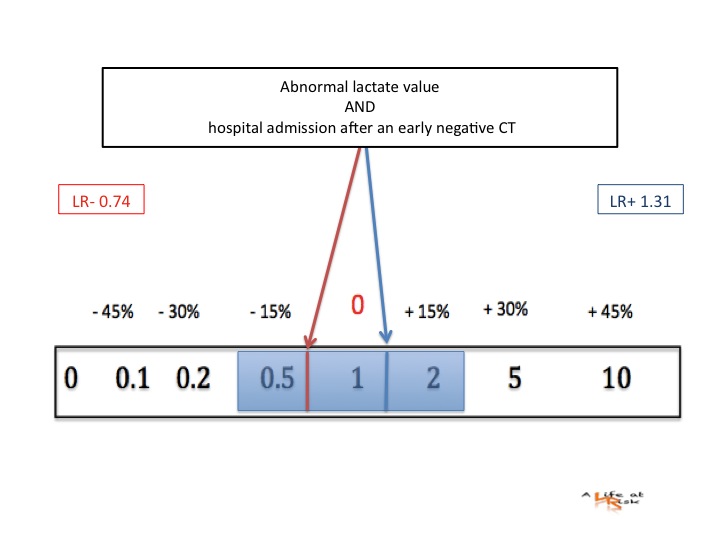
After 15 minutes, the patient returns to the ED, TC is negative, the patient feels better, the nurse says that the ABG is abnormal, pH is 7.5 and lactate level is 4.
Do abnormal ABG and/or SL change disposition after a negative CT?
Conclusion
The routine testing of ABG and lactate for a blunt trauma is unnecessary if the patient is stable and perform an early negative CT.
When are this tests necessary ? When the patient is instable, or when an hospital admission is necessary despite the CT results.
On the other hand puncture of the radial or inguinal artery is a painful procedure with risk of complications.
It is time to change our trauma protocol?
Bibliography
T Vohra
Abnormal arterial blood gas and serum lactate levels do not alter disposition in adult blunt trauma patients after early computed tomography.
West J Emerg Med, vol XIV n 3 May 2013 pagg 212-217
J L Isenhour
Advances in abdominal trauma.
Emerg Med Clin N Am 25 2007 pagg 713-723