A 80 YO man with a history of hypertension presents to the ED complaining of abdominal pain. He felt well until 8 hours ago, when he developed diffuse abdominal pain. The patient is afebrile, tachicardic, BP is 180/100 his lungs are clear, ECG shows no changes suggestive of ischemia. There is diffuse abdominal rigidity.
In another room there is a 22 yo girl with abdominal pain started two days before. She is febrile (38°C) and tachicardic, blood pressure is 120/80, her abdomen is soft. The cough test is positive, but rebound is negative.
In the 3rd room there is a 48 yo patient. Come in -says the nurse- this abdomen is like a board.
Where is peritonitis?
Conclusion
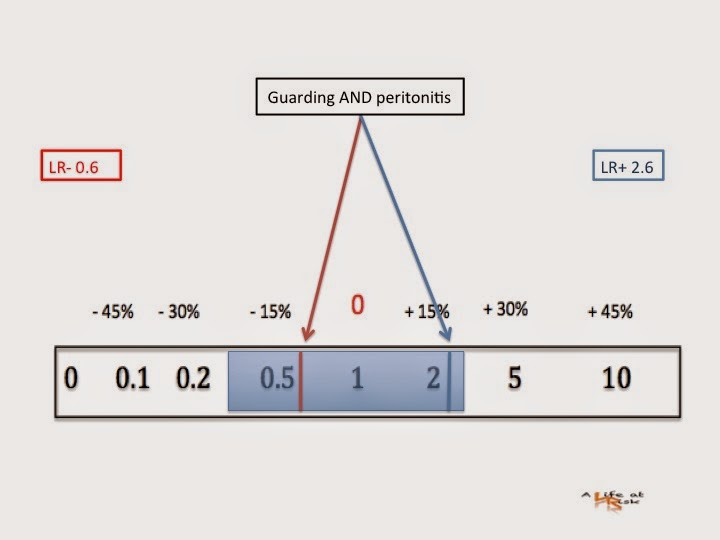
Determining the presence or absence of peritonitis is a primary objective of the abdominal examination. All the methods alone are inaccurate. Thoracic inflammatory process adjacent to the diaphragm, a voluntary contraction of the abdominal wall in apprensive patients, a rough painful examination, may be misleading. But what is more interesting is that no test alone is useful in ruling out a diagnosis of peritonitis. Furthermore a gentle percussion is as inaccurate as the rebound test is, but it saves unnecessary pain.
Bibliography
R McNamara
Approach to acute abdominal pain.
Emerg Med Clin N Am 2011 29 159-173
S McGee
Abdominal pain and tenderness
Evidence based physical diagnosis Saunders Ed. 2007.