It’s a busy Monday morning in ED.
A doctor at the phone – calls the nurse – there’s a primary care physician.
Hi – says a voice on the other side – I’m in a patient’s home.
He’s a 40 yo man with dyspepsia, his wife refers weight loss of about 10 Kg in the last three months. He is pale, but not tachicardic, abdomen is treatable, on rectal examination I find normal stool.
I’m warried he probably has a gastric cancer, Is it possible to schedule an urgent gastroscopy for this morning?
Conclusion
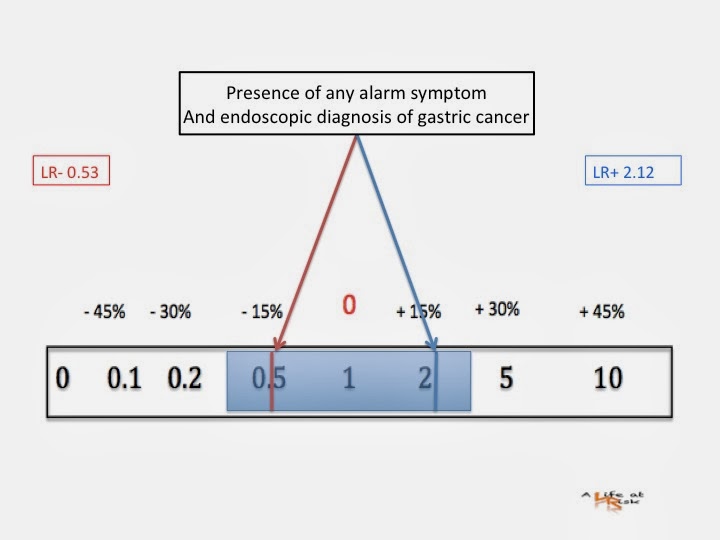
We all know the “alarm symptoms” that identify patients at high risk for gastric cancer: weight loss, vomiting, anemia, dysfagia, blood in stools, palpable abdominal mass. Guidelines reccomend urgent endoscopic investigation for patients of any age with dyspepsia when presenting with any of this red flags.
The above picture is clear: alone the presence of any high risk symptom is a poor predictor of gastric cancer. On the other hand the absence of those alert features doesn’t esclude the presence of disease.
Also when a patient with gastric cancer presents this symptoms this is indeed alarming.
Bibliography
Dyspepsia:management of dyspepsia in adults in primary care.
Clinical Guideline 17
Wallace MB
Age and alarm symptoms do not predict endoscopic findings among patients with dyspepsia: a multicentre database study.
Gut 2001; 49: pagg 29-34.
Maconi G
Role of symptoms in diagnosis and outome of gastric cancer.
World J Gastroenterol 2008 Feb 28 14(8) pagg 1149-1155.